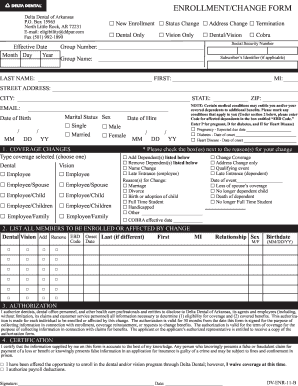
delta dental appeal form
Personal Representative Form Use this form if you want another person to represent you when making oral health care decisions. ASO contract addendum for HIPAA privacy and security.

Delta Dental Of Connecticut Delta Dental Of Connecticut
Through our national network of Delta Dental companies we offer dental coverage in all 50 states Puerto Rico and other US.
. Findings from the Delta Dental-commissioned research of 2000 US. Healthy Smile Healthy You enrollment. Backof this packet is a form that your provider may Your provider could also send a letter or make up a form with similar information Your treating provider must send the certification and.
You can file a grievance by doing one of the following. Delta Dental HIPAA Form 14b ASO Groups. Our mission is to improve lives by promoting optimal oral health.
View additional forms by logging in to your secure member portal. CLAIMS APPEALS SHOULD BE SENT TO THE STREET ADDRESS BELOW NOT THE PO BOX. Delta Dental of Arizona is a part of Delta Dental Plans.
Delta Dental of Arkansas. See member forms including notice of privacy practices. This form is not needed for.
Use this form to update the status of your practice as a DeltaCare provider. How Do I File a Grievance. Delta Dental of Kansas is a part of Delta Dental Plans Association.
Call toll-free at 1-866-864. Dba Delta Dental of Arizona. Find solutions that make it easier to manage your practice like benefit information and claims status.
Delta Dental of Arizona 5656 W. Adults and parents of children ages 12 and younger illuminate what they thought about their oral health and what. THE PO BOX IS FOR CLAIMS ONLY.
You may use this form to tell your benefits administrator you want to appeal a denial decision. Delta Dental requires providers use a resubmission request by selecting that option on this form to resubmit claims for clerical corrections or to provide additional information to support the. These Participation Review Panel Procedures are incorporated by.
The Appeal Request Form must be received by Delta Dental DDKS within 180 calendar days from the date of the original adverse benefit determination or the corresponding remittance. DELTA DENTAL OF ARKANSAS PARTICIPATION REVIEW PANEL PROCEDURES 1. Use this form to file out-of-network vision claims.
Signature of insured or authorized representative Date. Dentist Administrative Forms and Resources. Arizona Dental Insurance Service Inc.
DeltaCare Specialty Referral Form Use this form to refer your patient to a specialist. Delta Dental PPO participation packet request. Locum tenens provider form.
Delta Dental HIPAA Form 14a Risk Groups.

Delta Dental 101

Contact Us

Sample Letters Of Appeal To Dental Insurance Lovetoknow
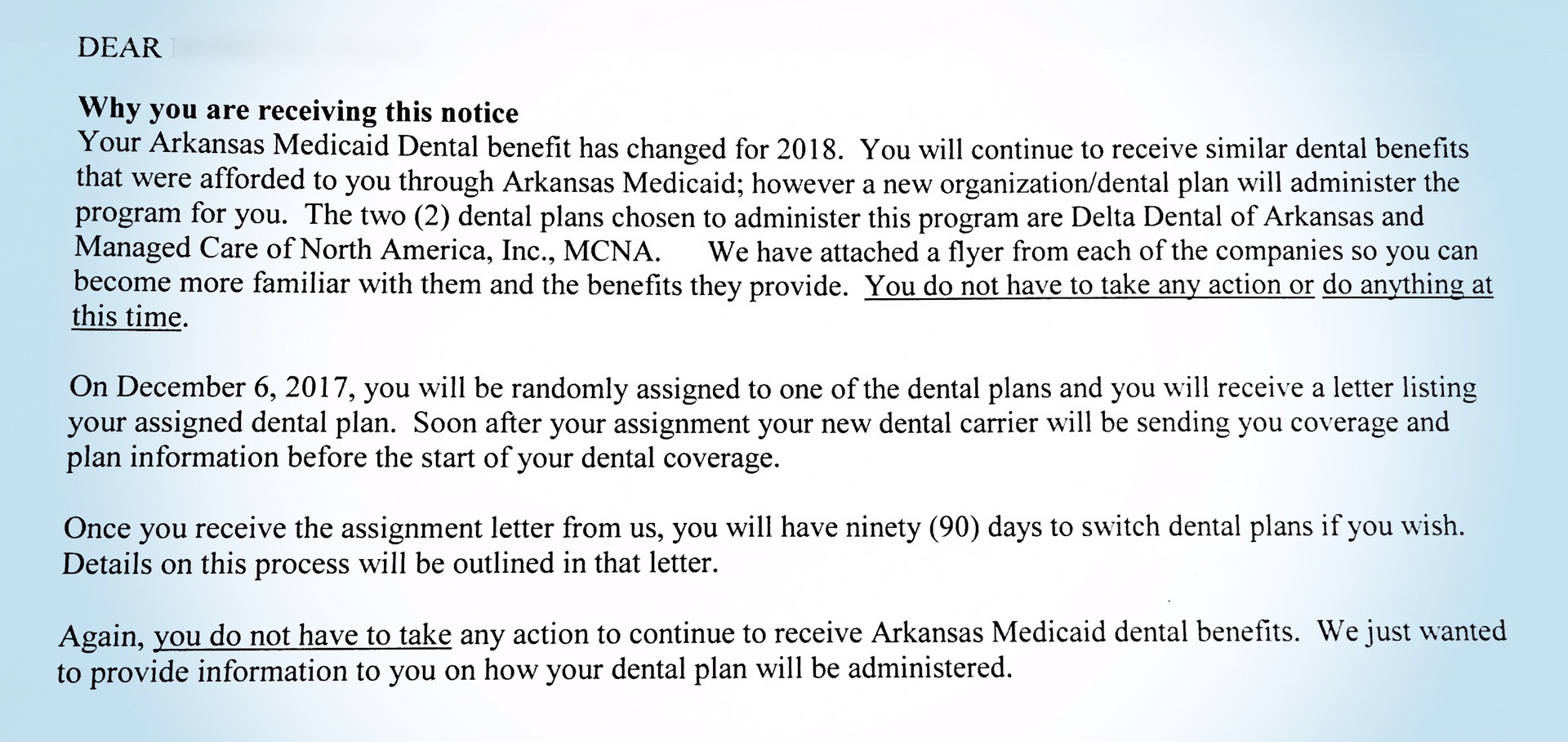
Patient Medicaid Saves Lives

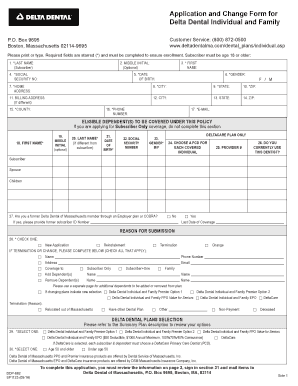
Fillable Online Disabled Dependent Application Delta Dental Massachusetts Form Fax Email Print Pdffiller

Dental Benefits State Of New Hampshire Human Resources
Delta Dental

Claim Form Delta Dental Insurance

Delta Dental Goes Mockumentary Style For Long Live Smile Power Pr Week

Forms Resources Deltadentalok
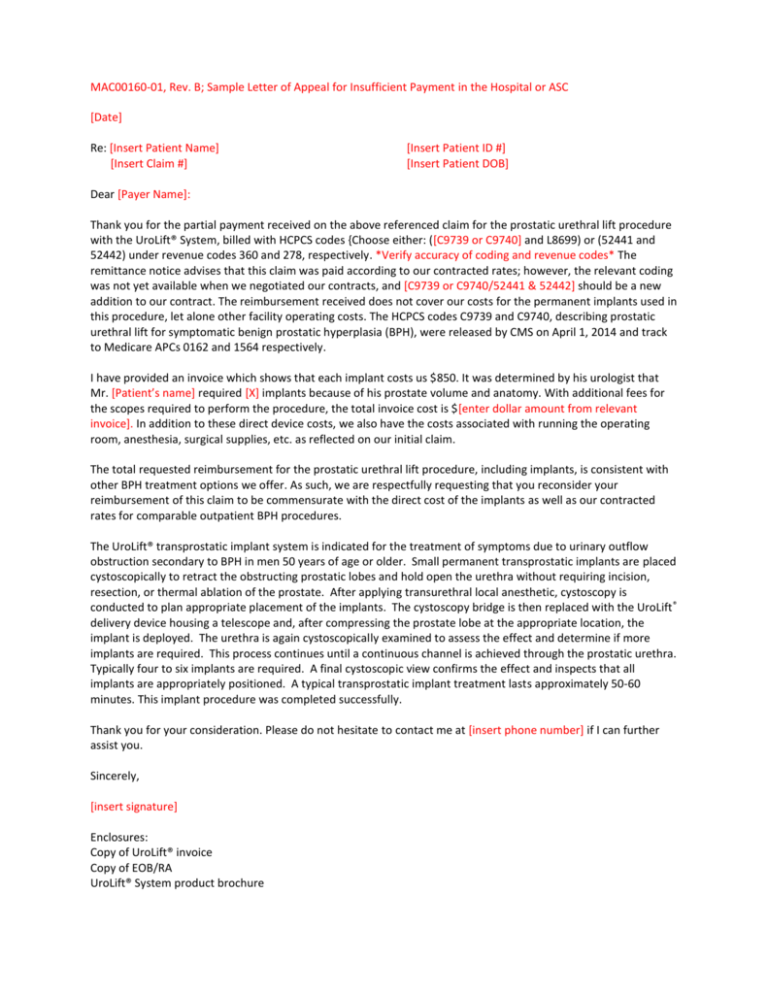
Sample Letter Of Appeal For Insufficient Payment Hospital

Dental Insurance Appeal Letter Template With How To Instructions
Delta Dental Of Ar Form Fill Out And Sign Printable Pdf Template Signnow

Delta Dental Of Arkansas Claims Address Fill Online Printable Fillable Blank Pdffiller

Provider Forms Resources Delta Dental Of Arkansas

News Release Delta Dental Of Wisconsin

State Of Wisconsin Etf Delta Dental Of Wisconsin Contact Us
Dental Insurance Gives Peace Of Mind According To Delta Dental Study

Providers